

This Won’t Hurt Me A Bit
C-Collars and Other Defensive Medical Rituals

In trauma care, few interventions are as reflexive as the application of a cervical collar. The patient arrives. The collar goes on. It is done quickly, almost automatically, as though it were a prerequisite for evaluation rather than a decision requiring justification. The practice is so ingrained that it often escapes scrutiny. Yet when examined closely, the cervical collar reveals something uncomfortable about modern medicine. It persists not because of strong evidence, but because of strong incentives.



The rationale appears straightforward. A patient with a potential cervical spine injury should have the neck immobilized to prevent further damage. This logic is intuitive and has been repeated for decades. It feels cautious, prudent, and safe. But intuition is not evidence, and the evidence for routine cervical immobilization is remarkably thin.
A Cochrane review examining spinal immobilization in trauma patients found no randomized controlled trials demonstrating that the practice improves neurologic outcomes, and concluded that there is insufficient evidence to support its routine use.1 The absence of high-quality evidence is a reflection of how deeply ingrained the practice had already become before modern standards of evaluation were applied. The most frequently cited comparative study, examining trauma systems in Malaysia, where immobilization was not routinely practiced, and New Mexico, where it was, found no reduction in neurologic injury with immobilization and in fact reported less neurologic disability among patients who were not immobilized.2 While not definitive, such findings directly challenge the intuitive premise that immobilization prevents secondary spinal cord injury.
At the same time, the harms of cervical collars are well documented. They increase intracranial pressure in patients with head injury, complicate intubation and advanced airway management, and impair respiratory mechanics.3 Prolonged use is associated with pressure ulcer formation and patient discomfort, particularly in populations for whom proper fit is difficult to achieve.4
These are not rare or theoretical complications. Rigid collars are frequently inapplicable in the patients most likely to present after trauma: the elderly patient with cervical kyphosis for whom proper fit is anatomically impossible, or the obese patient in whom the device provides no meaningful restriction of motion whatsoever. In the agitated patient with head injury, forced compliance with a rigid collar may itself provoke the very cervical movement the device is meant to prevent. The harms are concrete and documented; the benefits remain unproven.
It is therefore notable that several developed systems have already begun to move away from routine immobilization. Guidelines in the United Kingdom and elsewhere now emphasize selective spinal motion restriction rather than universal application of rigid collars.5 The persistence of routine immobilization in the United States, despite weak evidence of benefit and clear evidence of harm, suggests that forces other than patient outcomes are driving the practice.
To understand why, one must look beyond physiology and into incentives. The persistence of cervical collars is not a triumph of evidence-based medicine. It is a product of the highly litigious system in which American emergency physicians serve. It is purely an exercise in defensive medicine.
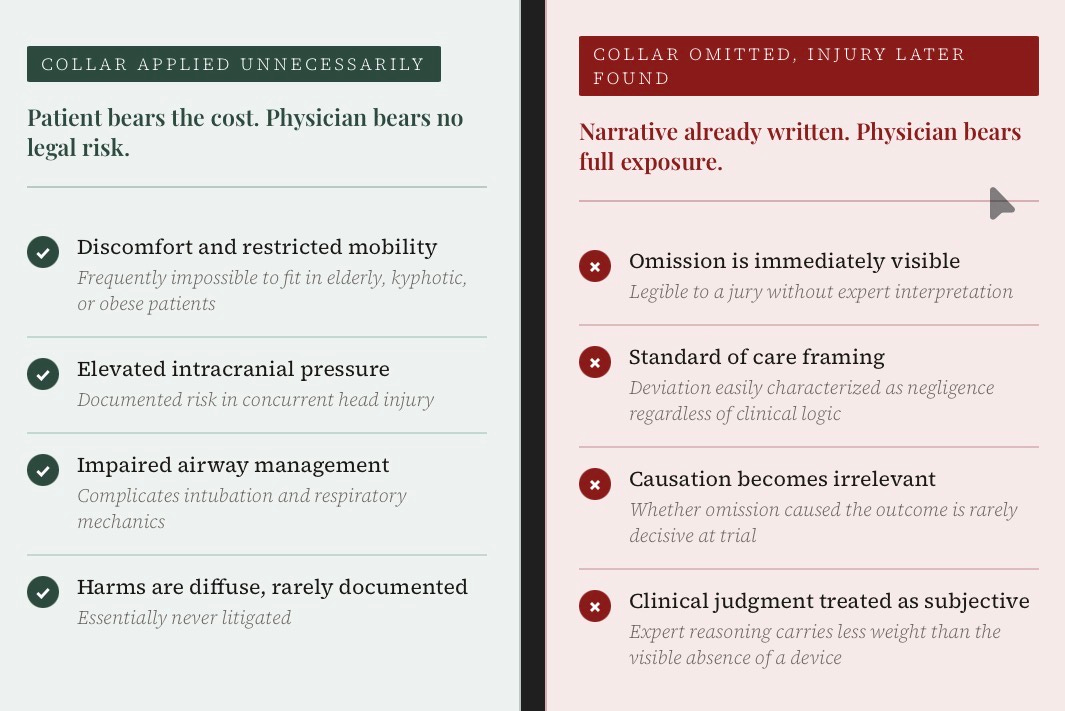
The physician evaluating a trauma patient faces a familiar asymmetry. If a collar is applied unnecessarily, the patient experiences discomfort and perhaps minor harm. These consequences are diffuse, rarely documented, difficult to prove, and therefore essentially never litigated. If a collar is not applied and the patient is later found to have a cervical spine injury, the consequences are entirely different. Even if the omission had no causal role in the outcome, the narrative is already written. A simple intervention was not performed. Standard of Care was not upheld. A catastrophic injury followed. The case is a slam dunk.
This asymmetry drives behavior. It is not that physicians believe strongly in the efficacy of cervical collars. It is that the legal risk of omission overwhelms the clinical ambiguity of benefit. The collar becomes a form of malpractice insurance, worn by the patient but purchased by the physician.
The legal pressure surrounding cervical spine injuries is real. Missed or delayed diagnosis of cervical spine trauma has long been recognized as a recurring source of malpractice litigation, often involving severe and irreversible neurologic outcomes.6 In such cases, the clinical nuance of whether immobilization would have altered the outcome is rarely the central issue. What matters is that a recognizable precaution was omitted. The absence of a cervical collar is easily framed as a deviation from standard practice, regardless of whether its application would have provided any meaningful protection. This dynamic is reinforced by a broader malpractice environment in which physicians routinely report ordering interventions primarily to reduce liability exposure rather than to benefit the patient.7 Even as professional organizations move toward more selective approaches to spinal motion restriction, they acknowledge that medicolegal concerns remain a significant barrier to change.8 The result is a system in which the visible act of precaution carries more legal weight than its clinical value.
The cervical collar is not unique. It is simply one of the most visible examples. Similar patterns appear throughout emergency care. Patients are placed on telemetry without clear indication, not because monitoring is expected to change management, but because the absence of monitoring is difficult to defend if an arrhythmia is later discovered. Rigid backboards, long known to cause pain and pressure injury, persisted for decades after their benefit was questioned, sustained more by protocol than by evidence. Even clinical decision tools, designed to support judgment, are often repurposed as documentation. Scores such as HEART, Wells, PESI, CURB-65, and NEXUS are frequently applied not to guide a decision, but to justify one already made, creating a record that the appropriate pathway was followed. Diagnostic testing follows the same logic. Low-risk patients undergo stress testing or coronary CT not because these tests meaningfully reduce the risk of myocardial infarction in that population, but because a normal result is legible reassurance in the chart. In each case, the intervention persists not because its benefit is clear, but because its omission is visible in retrospect.
This is particularly striking because physician judgment alone often performs remarkably well. In many studies, clinician gestalt rivals formal risk stratification tools in its ability to rule in or rule out serious disease. For example, one prospective study comparing physician gestalt to the HEART score in undifferentiated emergency department chest pain found no significant difference in overall diagnostic accuracy between the two approaches.9 Experienced physicians are reliably able to identify low-risk patients with accuracy comparable to that of the algorithms and tests later used to validate the decision. Yet gestalt alone is not considered defensible. A physician may accurately recognize that a patient is not suffering from acute coronary syndrome, pulmonary embolism, or cervical spine injury, but clinical judgment without objective documentation carries little legal protection. The test, the score, and the protocol are therefore not merely diagnostic instruments. They are evidentiary ones. In the courtroom, the physician’s expertise is often treated as subjective intuition, while the algorithm and the scan are treated as proof of diligence and concern. The irony is that both may arrive at the same conclusion, but only one reliably protects the doctor. A system that treats clinical expertise as legally inferior to algorithmic output does not merely inconvenience physicians; it communicates to them that their judgment is not worth cultivating.
Other countries, operating in less adversarial legal environments, have translated this evidentiary skepticism into formal policy. The United Kingdom’s NICE guidelines, updated in 2016, replaced the presumption of universal collar application with a structured clinical decision framework: patients are assessed using the Canadian C-spine Rule, and immobilization is applied selectively based on documented risk factors, not reflexively applied to every patient with a plausible mechanism of injury.10 Norway went further still. Its 2016 national prehospital guidelines explicitly recommended against routine collar use, proposing instead a tiered approach in which manual in-line stabilization, head blocks, and selective collar application are deployed based on clinical assessment, with penetrating trauma patients explicitly excluded from immobilization altogether.11 The principle underlying both frameworks is the same: a trained clinician, applying a validated decision tool, can identify which patients require immobilization and which do not, and the absence of a rigid collar in the latter group does not represent negligence. It represents judgment. The difference between these systems and the American one is not that physicians abroad are less concerned about patient safety. It is that their legal and professional environments allow clinical judgment to carry moral and institutional weight, rather than treating it as a liability to be insured against with hardware.
In the United States, that fear is ever-present. It shapes decisions in ways that are often invisible to those outside the profession. Policy discussions about healthcare costs frequently focus on administrative overhead, pharmaceutical pricing, or insurance structures. These are real issues, but they overlook a quieter and more pervasive force. The constant anticipation of litigation alters behavior at the bedside. It encourages interventions that are legally defensible rather than medically necessary.
Cervical collars are a particularly clear example because they are so visible. One can see them in every trauma bay, on every stretcher, on nearly every patient with even a remote possibility of injury. They are a physical manifestation of a legal environment that rewards excess caution when that caution is easy to explain, regardless of its clinical value.
When a practice persists despite weak evidence and known harms, one must ask what sustains it. In this case, the answer lies not in medicine but in law. The broader point is that defensive medicine is a structural feature of the system. It operates continuously, shaping thousands of small decisions that accumulate into significant cost and complexity. Many of these decisions, like the application of a cervical collar, appear minor in isolation. Collectively, they represent a substantial distortion of medical practice.
The system does not reward restraint. It punishes it. A physician who exercises judgment and omits an unnecessary intervention assumes a risk that is not shared by the physician who applies it reflexively. The result is predictable. Excess becomes standard, and deviation from excess becomes liability.
Any efforts to control healthcare costs that do not address the legal environment are destined to fall short. As long as physicians are judged not only by what they do, but by how their actions can be reconstructed in a courtroom, the incentive will be to do more rather than less. The marginal test, the precautionary intervention, the unnecessary device will continue to proliferate.
For now, the collar stays on, but it does not protect who it claims to.
This essay is the third of a series on defensive medicine.
Part 1: The Price of Torts
Part 2: The Alienated Patient
Kwan I, Bunn F. Spinal immobilisation for trauma patients. Cochrane Database Syst Rev. 2001;(2):CD002803. Updated 2009. doi:10.1002/14651858.CD002803
Hauswald M, Ong G, Tandberg D, Omar Z. Out-of-hospital spinal immobilization: its effect on neurologic injury. Acad Emerg Med. 1998;5(3):214–219. doi:10.1111/j.1553-2712.1998.tb02615.x
Kolb JC, Summers RL, Galli RL. Cervical collar-induced changes in intracranial pressure. Am J Emerg Med. 1999;17(2):135–137. doi:10.1016/S0735-6757(99)90035-7
Totten VY, Sugarman DB. Respiratory effects of spinal immobilization. Prehosp Emerg Care. 1999;3(4):347–352. doi:10.1080/10903129908958966
Ackland HM, Cooper DJ, Malham GM, Kossmann T. Factors predicting cervical collar-related decubitus ulceration in major trauma patients. Spine. 2007;32(4):423–428. doi:10.1097/01.brs.0000255077.10308.95
National Institute for Health and Care Excellence (NICE). Spinal injury: assessment and initial management (NG41). Published February 2016. https://www.nice.org.uk/guidance/ng41
Fischer PE, Perina DG, Delbridge TR, et al. Spinal motion restriction in the trauma patient: a joint position statement. Prehosp Emerg Care. 2018;22(6):659–661. doi:10.1080/10903127.2018.1481476
Davis JW, Phreaner DL, Hoyt DB, Mackersie RC. The etiology of missed cervical spine injuries. J Trauma. 1993;34(3):342–346. doi:10.1097/00005373-199303000-00006
Platzer P, Thalhammer G, Ostermann R, et al. Delayed or missed diagnosis of cervical spine injuries. Spine. 2006;31(6):E182–E185. doi:10.1097/01.brs.0000202767.78529.5a
Studdert DM, Mello MM, Sage WM, et al. Defensive medicine among high-risk specialist physicians in a volatile malpractice environment. JAMA. 2005;293(21):2609–2617. doi:10.1001/jama.293.21.2609
Jena AB, Seabury S, Lakdawalla D, Chandra A. Malpractice risk according to physician specialty. N Engl J Med. 2011;365:629–636. doi:10.1056/NEJMsa1012370
Fischer PE, Perina DG, Delbridge TR, et al. Spinal motion restriction in the trauma patient: a joint position statement. Prehosp Emerg Care. 2018;22(6):659–661. doi:10.1080/10903127.2018.1481476
Visser A, Wolthuis A, Breedveld R, ter Avest E. HEART score and clinical gestalt have similar diagnostic accuracy for diagnosing ACS in an unselected population of patients with chest pain presenting in the ED. Emerg Med J. 2015;32(8):595–600. doi:10.1136/emermed-2014-203798
National Institute for Health and Care Excellence. Spinal Injury: Assessment and Initial Management. NICE Guideline NG41. London: NICE; February 17, 2016. https://www.nice.org.uk/guidance/ng41
Kornhall DK, Jørgensen JJ, Brommeland T, et al. The Norwegian guidelines for the prehospital management of adult trauma patients with potential spinal injury. Scand J Trauma Resusc Emerg Med. 2017;25:2. doi:10.1186/s13049-016-0345-x